 By Dennis Gallagher, MA, MPA Associate Teaching Professor Drexel University, Dornsife School of Public Health Department of Health Management and Policy After almost three full years of experience with the Affordable Care Act (ACA), it is clear that changes to the law are necessary if it is to sustain the good things that it has achieved to date. Even bigger changes are called for if it is to attain broader goals of expanding access to affordable health care, constrain the growth in costs, and improve the health of the U.S population. Unfortunately, in the super-charged world of American politics, the chances for meaningful and effective changes to the ACA seem remote, no matter which candidate wins the presidential election.
Let’s break that sad scenario into two parts. If Hillary Clinton becomes President, we should assume that she will advocate for the major changes to the ACA that are in the Democratic party election platform. The most important change, which is also the one least likely to happen, is the creation of a public plan option for persons residing in areas of the country where there are very few or no insurance options in the healthcare marketplace. The argument for the public plan option is to assure access to health insurance and gain the benefits of competition between insurance plans. But the essential Republican philosophical point of opposition to the ACA (beyond the simple political fact that it is associated with President Obama and the Democrats) is that it establishes a large, critical regulatory role for the Federal government in the functioning and oversight of the U.S. health system. Creating a new public plan option would expand the Federal government’s role in, and responsibility for, health care financing. Republican opposition to the public plan option was severe in 2009 when negotiations were underway to draft what would become the ACA, and Democrats in Congress dropped it from consideration when the law was finally drafted and enacted. At best, it’s hard to imagine the public plan option getting a serious hearing in Congress in the next several years, even if the Democrats achieve a majority in the Senate. If Donald Trump becomes President, we should assume that legislative efforts to repeal and replace the ACA with an alternative Republican program, or set of programs, would take on new life and heightened energy. The Republican legislative approach would likely retain some popular elements of the ACA, like guaranteed issuance of health insurance regardless of pre-existing conditions. It would also eliminate the individual mandate to purchase health insurance and employer mandates to provide coverage, expand the role of individual/family health savings accounts to help pay for the purchase of private insurance, offer tax credits for people without employer-based coverage to offset the cost of purchasing health insurance, and create state-based, subsidized high-risk pools for people with expensive medical conditions. A Republican approach would also eliminate the expansion of Medicaid coverage for low-income adults, and instead transform the Medicaid program by giving states the authority to decide how Federal funds would be spent, while also capping Federal funding, annually. The Republican plan would also eliminate the essential health benefits that all individual insurance plans must now provide, allowing instead for the sale and purchase of low cost, minimal benefit, “mini-medical” plans across state lines. Although a President Trump would likely have a Republican majority in both houses of Congress, attempts at repealing the ACA and replacing it instead with a set of programs like those proposed by Republican Congressmen and articulated in the Republican party platform might well be blocked in large measure by the sizable Democratic minority in the Senate. It would take 60 Senators to vote to approve this legislation, and it seems unlikely that Senate Democrats would agree to support these measures – most of which have either been opposed by Democrats for decades – like “block granting” Medicaid -- or which have failed in the past to achieve the desired ends – like state-based “high-risk pools.” So, what can we expect will happen to the ACA after the election? The easy and most probable answer is – not much, certainly not in the short term. Republicans currently have a lawsuit (US House of Representatives vs Burwell) in the works in an attempt to find that the Department of Health and Human Services exceeded its constitutional authority by using funds not appropriated by Congress to pay for cost-sharing subsidies for low-income persons covered by plans in the ACA marketplace. A May 2016 ruling in the D.C. District Court found in favor of the House and is now under appeal. A President Clinton and the Democrats would get little support – or attention -- from Republicans at least not until this court case is resolved in final. At best there might be efforts made afterward on the margins of the ACA, to address several requirements affecting small businesses and their employees. But such changes would be minimal. Congress would likely continue efforts to block appropriations for parts of the ACA, almost certainly ensuring that the ACA never fully achieves its reform potential and likely endangering its continuation because of growing instability in the health insurance market. On the other hand, a President Trump would have to find a way to overcome Democratic Senators who would otherwise block efforts to repeal and replace the ACA with Republican approaches. In that case, one might imagine a long, slow, ugly transition from the ACA to something like a Republican re-casting of it – a scenario that might be necessitated by (successful) Republican measures to strangle funding of key parts of the ACA, as part of the annual budget and appropriations process. What can we almost certainly NOT expect? Sadly, we should not expect true partisanship in reforming the U.S. health system. Health care will remain a battle ground no matter what the election brings.  by Meghan Smith, MPHc 2017 Note: Meghan wrote this piece before the November elections. She believes that it is crucial, now more than ever, to reach across the aisle, attend or host discussion forums, get outside your comfort zone, and open up new channels of communication so that diverse voices are heard and part of public health dialogue. Growing up in a rural town along the New York/New Jersey state border, I was surrounded by small farms, independently run grocery stores, hospitals, and physician practices. Although it was not geographically far from New York City it felt distinctly removed from the issues affecting that ubiquitous urban giant. Since my childhood, the town has changed with increased commercialization and altered demographics, but it still retains the rural atmosphere. This urban/rural divide persists throughout the United States as well, with the divide growing deeper every year. According to the 2010 US Census, 80.7% of the country’s population lived in urban areas, whereas only 19.3% of the population lived in rural areas. For urban areas, this represents a 12% increase in population since 2000. With more and more people moving from rural to urban areas, there is a shift in population density, allocation of resources, affordable housing, employment opportunities, and economic development. This is an issue affecting public health. As someone who is passionate about food policy, I have seen how the disparities between rural and urban are deeply impactful. I recently completed a summer research assistant position with the Center for a Livable Future at Johns Hopkins University. My team worked specifically on connecting with food policy councils throughout North America, connecting councils with each other, and offering resources and technical assistance to help councils create a more just and sustainable food system. This included working with councils at the state, regional, and local level. The majority of councils are dealing with the same food-related issues, yet the manner in which councils approach these issues differs vastly depending on their community and region. For example, food access is an issue facing most councils, as well as most of the United States, however, that issue looks different from an urban or rural perspective. In an urban area, a barrier to food access may be the lack of a full-service grocery store, offering fresh produce, in the neighborhood. However, this urban area may operate a public transportation system with routes to a grocery store in a different neighborhood so that those in the area have the means to get to and from a grocery store and their neighborhood. In a rural area, there may be multiple full-service grocery stores, offering fresh produce, but no public transit system. How are those living in this area without cars expected to buy groceries? Another issue is food production. This looks very different for urban and rural communities. In urban communities, there may be a desire to implement public policy which supports the revitalization of vacant lots into community gardens, or the preservation of land and rights for existing community gardens against urban development. In rural areas, there may be a need to develop policy which incentivizes the preservation of large swaths of land for small family farms, fruit and vegetable farms, free-range animals, over the interests of large, multi-national corporations (commodity farming, factory farming, etc.). In my time at the Dornsife School of Public Health, and at the Center for a Livable Future, professors, faculty, mentors, and fellow students have consistently emphasized the importance of community input. There is value in listening to stakeholders, engaging them in the conversation, and working to include their input in program and policy implementation. This extends to bridging the rural and urban divide. It is increasingly important to listen to stakeholders in all types of communities, to take into account how policy and programs impact the two areas, especially at the state, county, and regional level. A policy in urban Philadelphia may have a direct effect on Lancaster County. The United States is a patchwork quilt of communities, each with its own unique characteristics and people. It is necessary to value that uniqueness in order to create a healthier and stronger population. 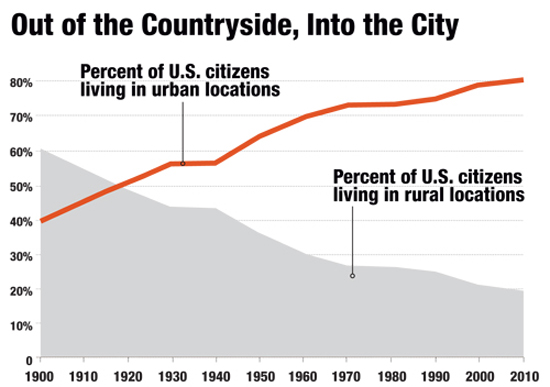  by Jesse Lloyd Goldshear, MPH Research Coordinator, Social Media and Health Innovation Lab, University of Pennsylvania 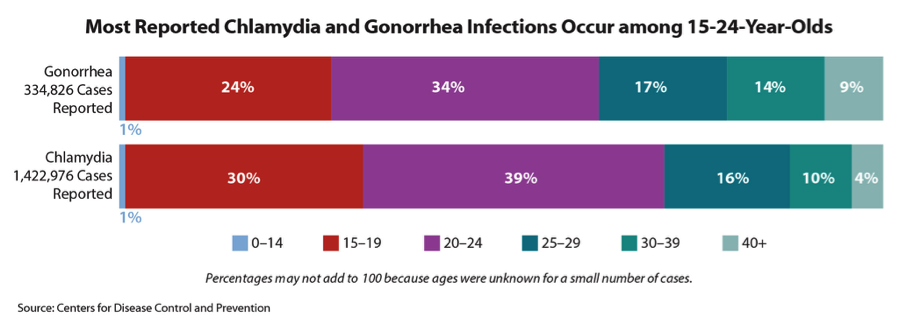 In 2014 the CDC reported almost 2 million new cases of the top three sexually transmitted infections (STIs), chlamydia, gonorrhea, and syphilis – all increases from the year before. Adolescents and young adults (prime users of social media platforms) accounted for almost two-thirds of these new cases of gonorrhea and chlamydia and have the highest risk of becoming infected.[i] The CDC also reports that in 2014 there were nearly 50,000 new HIV diagnoses, about one-fifth of which were diagnosed in patients in the same age-range.[ii] A new diagnosis of a STI or HIV can not only be scary for many individuals, but can also be accompanied by feelings of shame, lack of self-worth, and perceived stigma and isolation from others. The effects of stigma surrounding STI and HIV infection cannot be understated, especially when compounded with racial, ethnic, or sexual minority status. Research has shown that stigma and shame surrounding infection can become barriers to prevention and treatment: people may not seek testing, even after sex they knew to be risky, due to social stigma surrounding these infections.[iii] Feelings of shame are especially high among HIV-positive individuals who are also racial/ethnic minorities. This stigma can lead to a lower quality of life, independent of other factors.[iv] Additionally, HIV stigma is associated with lower self-reported physical and mental health status, and lower adherence to medication regimens.[v] Stigma, shame, and fear of a partner’s reaction to a diagnosis may motivate people to not disclose their status resulting in higher rates of infection transmission, especially among marginalized groups and vulnerable populations. The rise of social media platforms in the last decade has connected more people than ever before, enabling almost-instantaneous sharing of information between individuals, communities, organizations, and governments. Already, we’ve seen how these platforms have been used in a variety of situations where rapid communication between large groups was beneficial. In 2013, Twitter overflowed with information about the Boston Marathon bombing, well before official media and emergency channels were able to spread word about the tragedy.[vi] The following year, Facebook launched a feature that let users notify friends and family of their status during a natural disaster in their area.[vii] This ability to communicate and transmit information rapidly has drawbacks however: Twitter was recently the platform-of-choice for coordinated racist and misogynistic attacks against actress Leslie Jones, forcing her off of the social media network.[viii] But how are these platforms important for public health? More specifically, how are they important in the fight against stigma that surrounds STI and HIV infection? Social media platforms have already become tools for rapid dissemination of public health news, research, and programming. Groups such as the CDC, the Philadelphia Department of Public Health, and Drexel University Dornsife School of Public Health, all maintain constant online presences on Twitter. Research groups, such as the Social Media and Health Innovation Lab at University of Pennsylvania and the Center for Digital Health Innovation at University of California, San Francisco, look into how social media can improve the health of populations and how communities talk about health issues on social media platforms. Studies like this one [ix] utilize social media platforms to reach key populations that were once considered “hard-to-reach.” Planned Parenthood uses Twitter to advocate for a variety of causes surrounding HIV/AIDS and sexual health. Outside of HIV/AIDS and STI advocacy, Planned Parenthood uses Twitter to advocate for women’s reproductive rights, and racial, gender, and sexual equality. They are just one example of large organizations advocating for a variety of public health causes around the world using social media.  Now however, we’re seeing social media become a tool for advocacy and activism specifically on the themes of HIV/AIDS and STIs. Groups such as POZ magazine, Black Women’s Health Imperative, and the International AIDS Society post daily to Twitter, urging their audience to speak up in support of HIV/AIDS advocacy. Groups like these also maintain an active Instagram presence, sharing images of support, outreach posters and fliers, and image-based calls to action. These organizations’ use of social media is and will be key to ending the stigma and shame that surrounds a diagnosis with HIV or an STI. Outside of organizational efforts however, individual efforts will be crucial to ending this stigma at a societal level. As of this writing, there have been 21 Twitter accounts (organizations and individuals) which used the hashtag #HIVstigma in a tweet in the past four days, meaning almost 46,000 other Twitter users could have seen this message in that time period.[x] Campaigns to end stigma that rely on social media-driven efforts have the potential to reach massive amounts of people in short periods of time due to the nature of social networks. Started by organizations, these campaigns must be driven by individual users within their own social networks. These future campaigns can take multiple approaches to ending HIV and STI stigma, ranging from raising awareness of the prevalence of these infections, to dispelling myths about the people who acquire them, to spreading personal stories of people who live with them. Some campaigns may be able to utilize a multi-pronged approach, while others will benefit from using a more focused approach.  Informal groups of Facebook and Twitter users such as Black Twitter[xi] are already driving advocacy on a variety of public health-related issues including systemic racial injustice in the US criminal justice system and sexual assault of women-of-color, among many others.[xii] The hard-driving and real-time advocacy of networks like Black Twitter gain massive mainstream media attention and have brought issues into the broader public spotlight like they might not have been a decade ago. The social-justice orientation of this and similar networks will be instrumental in the success of future attempts to end HIV and STI stigma via social media networks.
As a public health community made up of public- and private-sector health care workers, university educators, students, and advocates, we must focus on bringing an end to the life-threatening stigma and shame that surrounds a positive HIV or STI diagnosis. In this new era of social media a large part of our efforts must focus on how to leverage the influence of individuals, networks, and organizations to promote this goal online. Traditional boots-on-the-ground advocacy must be supplemented with social media savvy; only then we will be able to foster the change we wish to see. ----------------- [i] http://www.cdc.gov/nchhstp/newsroom/2015/std-surveillance-report-press-release.html [ii] http://www.cdc.gov/hiv/statistics/overview/ [iii] http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4334654/ [iv] http://www.sciencedirect.com/science/article/pii/S1055329009000338 [v] http://link.springer.com/article/10.1007/s10461-008-9455-4 [vi] http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3706072/ [vii] http://www.newsweek.com/facebook-launches-safety-check-feature-natural-disasters-277935 [viii] http://www.nytimes.com/2016/07/20/technology/twitter-bars-milo-yiannopoulos-in-crackdown-on-abusive-comments.html [ix] http://www.jmir.org/2014/4/e113/?trendmd-shared=0 [x] http://keyhole.co/realtime-rebuild/jRhSDc/HIVstigma [xi] http://gradworks.umi.com/36/68/3668450.html [xii] http://www.theatlantic.com/technology/archive/2015/04/the-truth-about-black-twitter/390120/ |
Who Can Contribute?Community Voice authorship is shared by diverse members of the Public Health and Philadelphia communities. Archives
March 2017
Categories |
 RSS Feed
RSS Feed
